Active drug substance: verapamil hydrochloride.
1 film coated tablet contains 240mg of verapamil hydrochloride.
Verapamil hydrochloride is a calcium ion influx inhibitor (slow channel blocker or calcium ion antagonist). The chemical name of verapamil hydrochloride is benzeneacetonitrile, α-[3-[{2-(3,4-dimethoxyphenyl) ethyl} methylamino] propyl]-3,4-dimethoxy-α-(1-methylethyl) hydrochloride. It has a molecular weight of 491.07 and the molecular formula is C27H38N2O4•HCl.
Verapamil hydrochloride is a calcium ion influx inhibitor (slow channel blocker or calcium ion antagonist). Verapamil hydrochloride is an almost white, crystalline powder, practically free of odor, with a bitter taste. It is soluble in water, freely soluble in chloroform, sparingly soluble in alcohol and practically insoluble in ether.
Excipients/Inactive Ingredients: Cellulose, Montan Glycol Wax, Macrogols (Type 400 and Type 6000), Magnesium stearate, Hypromellose, Povidone, Quinoline yellow, Indigo Carmine, Sodium alginate, Talc, Titanium dioxide, Ethanol anhydrous, Purified water.
Pharmacotherapeutic group: Selective calcium channel blockers with direct cardiac effects, phenylalkylamine derivatives. ATC-Code: C08DA01.
Pharmacology: Pharmacodynamics: Verapamil hydrochloride is a white or practically white crystalline powder. It is practically odorless and has a bitter taste. It is soluble in water, freely soluble in chloroform, sparingly soluble in alcohol and practically insoluble in ether. The chemical name of verapamil hydrochloride is benzeneacetonitrile, α-[3-[{2-(3,4-dimethoxyphenyl)ethyl}methylamino] propyl]-3,4-dimethoxy-α-(1-methylethyl) hydrochloride. It has a molecular weight of 491.07 and the molecular formula is C27H38N2O4 • HCl.
Mechanism of action and Pharmacodynamic effects: Verapamil inhibits the calcium ion (and possibly sodium ion) influx through slow channels into conductile and contractile myocardial cells and vascular smooth muscle cells. The antiarrhythmic effect of verapamil appears to be due to its effect on the slow channel in cells of the cardiac conductile system. Electrical activity through the sinoatrial (SA) and atrioventricular (AV) nodes depends, to a significant degree, upon calcium influx through the slow channel. By inhibiting this influx, verapamil slows AV conduction and prolongs the effective refractory period within the AV node in a rate-related manner. This effect results in a reduction of the ventricular rate in patients with atrial flutter and/or atrial fibrillation and a rapid ventricular response. By interrupting re-entry at the AV node, verapamil can restore normal sinus rhythm in patients with paroxysmal supraventricular tachycardias (PSVT), including Wolff-Parkinson-White (W-P-W) syndrome. Verapamil has no effect on conduction across accessory bypass tracts.
Clinical efficacy and safety: Verapamil does not alter the normal atrial action potential or intraventricular conduction time, but depresses amplitude, velocity of depolarization and conduction in depressed atrial fibers. In the isolated rabbit heart, concentrations of verapamil that markedly affect SA nodal fibers or fibers in the upper and middle regions of the AV node have very little effect on fibers in the lower AV node (NH region) and no effect on atrial action potentials or His bundle fibers. Verapamil does not induce peripheral arterial spasm nor does it alter total serum calcium levels. Verapamil reduces afterload and myocardial contractility.
In most patients, including those with organic cardiac disease, the negative inotropic action of verapamil is countered by reduction of afterload and cardiac index is usually not reduced, but in patients with moderately severe to severe cardiac dysfunction (pulmonary wedge pressure above 20 mmHg, ejection fraction less than 30%), acute worsening of heart failure may be seen. Peak therapeutic effects occur within three to five minutes after a bolus injection of verapamil. The commonly used intravenous doses of 5 to 10 mg verapamil hydrochloride produce transient, usually asymptomatic, reduction in normal systemic arterial pressure, systemic vascular resistance and contractility; left ventricular filling pressure is slightly increased.
Pharmacokinetics: Verapamil hydrochloride is a racemic mixture consisting of equal portions of the R-enantiomer and the S-enantiomer. Verapamil is extensively metabolized. Norverapamil is one of 12 metabolites identified in urine, has 10 to 20% of the pharmacologic activity of verapamil and accounts for 6% of excreted drug. The steady-state plasma concentrations of norverapamil and verapamil are similar. Steady state after multiple once daily dosing is reached after three to four days.
Absorption: Greater than 90% of verapamil is rapidly absorbed from the small intestine after oral administration. Mean systemic availability of the unchanged compound after a single dose of IR verapamil is 22% and that of SR verapamil approximately 33%, owing to an extensive hepatic first-pass metabolism. Bioavailability is about two times higher with repeated administration. Peak verapamil plasma levels are reached four to five hours after SR administration. The peak plasma concentration of norverapamil is attained approximately five hours after SR administration. The presence of food has no effect on the bioavailability of verapamil.
Distribution: Verapamil is widely distributed throughout the body tissues, the volume of distribution ranging from 1.8-6.8 L/kg in healthy subjects. Plasma protein binding of verapamil is approximately 90%.
Metabolism: Verapamil is extensively metabolized. In vitro metabolic studies indicate that verapamil is metabolized by cytochrome P450 CYP3A4, CYP1A2, CYP2C8, CYP2C9 and CYP2C18. In healthy men, orally administered verapamil hydrochloride undergoes extensive metabolism in the liver, with 12 metabolites having been identified, most in only trace amounts. The major metabolites have been identified as various N and O-dealkylated products of verapamil. Of these metabolites, only norverapamil has any appreciable pharmacological effect (approximately 20% that of the parent compound), which was observed in a study with dogs.
Elimination: Following oral administration, the elimination half-life is three to seven hours. Approximately 50% of an administered dose is eliminated renally within 24 hours, 70% within five days. Up to 16% of a dose is excreted in the feces. About 3% to 4% of renally excreted drug is excreted as unchanged drug. The total clearance of verapamil is nearly as high as the hepatic blood flow, approximately 1 L/h/kg (range: 0.7-1.3 L/h/kg).
Special Populations: Pediatric: Limited information on the pharmacokinetics in the paediatric population is available. Steady-state plasma concentrations appear to be somewhat lower in the pediatric population after oral dosing compared to those observed in adults.
Geriatric: Aging may affect the pharmacokinetics of verapamil given to hypertensive patients. Elimination half-life may be prolonged in the elderly. The antihypertensive effect of verapamil was found not to be age-related.
Renal insufficiency: Impaired renal function has no effect on verapamil pharmacokinetics, as shown by comparative studies in patients with end-stage renal failure and subjects with healthy kidneys. Verapamil and norverapamil are not significantly removed by hemodialysis.
Hepatic insufficiency: The half-life of verapamil is prolonged in patients with impaired liver function owing to lower oral clearance and a higher volume of distribution.
Toxicology: Preclinical safety data: Reproduction studies have been performed in rabbits and rats at oral verapamil doses up to 1.5 (15 mg/kg/day) and 6 (60 mg/kg/day) times the human oral daily dose, respectively, and have revealed no evidence of teratogenicity. In the rat, however, this multiple of the human dose was embryocidal and retarded fetal growth and development, probably because of adverse maternal effects reflected in reduced weight gains of the dams. This oral dose has also been shown to cause hypotension in rats. There are, however, no adequate and well-controlled studies in pregnant women.
The doses of Isoptin SR 240mg, individualized according to the severity of the disease, are to be taken regularly as prescribed by the physician. The film coated tablets are to be swallowed whole with some fluid, preferably with or shortly after meals. Unless otherwise instructed, the daily dose for adults is 1 film coated tablet in the morning (patients requiring particularly gradual blood pressure lowering should be started on half tablet taken in the morning). If after about 2 weeks of treatment a dose increase is found to be necessary the dose can be raised to a maximum of 2 film coated tablets daily (additionally 1 half to 1 film coated tablet in the evening after an interval of about 12 hours). On long-term treatment a daily dose of 480mg should not be exceeded; short-term dose increases are possible only when directed by the physician. For children and adults requiring smaller doses of verapamil, Isoptin 40mg and 80mg are available. In patients with impaired hepatic function the effect of verapamil is intensified and prolonged depending on the severity of the liver disease due to the diminished drug metabolism. In these cases dosage should be adjusted with special care starting with low doses (eg. in patients with hepatic cirrhosis with 1 tablet 40mg 2-3 times daily).
Special Population: Renal Impairment: Current available data are described in Precautions. Verapamil hydrochloride should be used cautiously and with close monitoring in patients with impaired renal function.
Liver Impairment: In patients with impaired liver function, metabolism of the drug is delayed to a greater or lesser extent depending on the severity of hepatic dysfunction, thus potentiating and prolonging the effects of verapamil hydrochloride. Therefore, the dosage needs to be adjusted with special caution in patients with impaired liver function and low doses should be given initially (see Precautions).
Method of administration: For oral use only.
Tablets should be taken without sucking or chewing, with sufficient liquid, preferably with or shortly after meals.
Clinical Manifestations: Hypotension, bradycardia up to high degree AV block and sinus arrest, hyperglycemia, stupor, metabolic acidosis and acute respiratory distress syndrome. Fatalities have occurred as a result of overdose.
Treatment: Treatment of verapamil hydrochloride overdose should be mainly supportive and individualized. Beta adrenergic stimulation and/or parenteral administration of calcium injection (calcium chloride) have been effectively used in treatment of deliberate overdosage with oral verapamil hydrochloride. Clinically significant hypotensive reactions or high-degree AV block should be treated with vasopressor agents or cardiac pacing, respectively. Asystole should be handled by the usual measures including beta adrenergic stimulation (e.g., isoproterenol hydrochloride), other vasopressor agents or cardiopulmonary resuscitation. Due to the potential for delayed absorption of the sustained release product, patients may require observation and hospitalization for up to 48 hours. Verapamil hydrochloride cannot be removed by hemodialysis.
Hypersensitivity to verapamil hydrochloride or to any of the inactive ingredients.
Cardiogenic shock.
Second or third degree AV block (except in patients with a functioning artificial pacemaker).
Sick sinus syndrome (except in patients with a functioning artificial pacemaker).
Congestive heart failure and/or severe left ventricular dysfunction (e.g. reduced ejection fraction of less than 35%, and/or pulmonary wedge pressure above 20 mmHg), unless secondary to a supraventricular tachycardia amenable to verapamil therapy.
Atrial fibrillation/flutter in the presence of an accessory bypass tract (e.g. Wolff-Parkinson-White, Lown-Ganong-Levine syndromes). These patients are at risk to develop ventricular tachyarrhythmia including ventricular fibrillation if verapamil hydrochloride is administered.
Acute myocardial infarction with complications (bradycardia, marked hypotension, left ventricular failure) and sinoatrial block.
Combination with Ivabradine (see Interactions).
Heart Block/First degree AV block/Asystole/Bradycardia (<50 beats/min): Verapamil hydrochloride affects the AV and SA nodes and prolongs AV conduction time. Use with caution as development of second- or third-degree AV block (contraindication) or unifascicular, bifascicular or trifascicular bundle branch block requires discontinuation in subsequent doses of verapamil hydrochloride and institution of appropriate therapy, if needed. Verapamil hydrochloride affects the AV and SA nodes and rarely may produce second- or third degree AV block, bradycardia, and, in extreme cases, asystole. This is more likely to occur in patients with a sick sinus syndrome (SA nodal disease), which is more common in older patients. Asystole in patients other than those with sick sinus syndrome is usually of short duration (few seconds or less), with spontaneous return to AV nodal or normal sinus rhythm. If this does not occur promptly, appropriate treatment should be initiated immediately. See Adverse Reactions.
Anti-arrhythmic and Beta blockers: Mutual potentiation of cardiovascular effects (higher-grade AV block, higher-grade lowering of heart rate, induction of heart failure and potentiated hypotension). Asymptomatic bradycardia (36 beats/minute) with a wandering atrial pacemaker has been observed in a patient receiving concomitant timolol (a beta-adrenergic blocker) eye drops and oral verapamil hydrochloride.
Digoxin: If verapamil is administered concomitantly with digoxin, reduce digoxin dosage. See Interactions.
Heart Failure: Heart failure patients with ejection fraction higher than 35% should be compensated before starting verapamil treatment and should be adequately treated throughout.
Hypotension: Hypotensive symptoms of lethargy and weakness with faintness have been reported following single oral doses and even after some months of treatment. In some patients it may be necessary to reduce the dose of verapamil hydrochloride.
HMG-CoA Reductase Inhibitors ("Statins"): See Interactions.
Neuromuscular transmission disorders: Verapamil hydrochloride should be used with caution in the presence of diseases in which neuromuscular transmission is affected (myasthenia gravis, Lambert-Eaton syndrome, advanced Duchenne muscular dystrophy).
Ventricular Tachycardia: The risk of inducing ventricular tachycardia cannot be excluded.
Other Special Populations: Renal impairment: Although impaired renal function has been shown in robust comparator studies to have no effect on verapamil pharmacokinetics in patients with end-stage renal failure, several case reports suggest that verapamil should be used cautiously and with close monitoring in patients with impaired renal function.
Verapamil cannot be removed by hemodialysis.
Liver impairment: Use with caution in patients with severely impaired liver function (see also Liver Impairment under Dosage & Administration).
Effects on ability to drive and use machines: Due to its hypotensive effect, depending on the individual response, verapamil hydrochloride may affect the ability to react to the point of impairing the ability to drive a vehicle, operate machinery or work under hazardous conditions. This applies all the more at the start of treatment when the dose is raised, when switching from another drug and in conjunction with alcohol. Verapamil may increase the blood levels of alcohol and slow its elimination. Therefore, the effects of alcohol may be exaggerated.
Pregnancy: There are no adequate and well-controlled study data in pregnant women. Verapamil crosses the placenta and has been measured in umbilical cord blood. Verapamil hydrochloride should not be given during pregnancy (especially in the first trimester) unless, in the physician's judgement, it is essential for the patient's well-being (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Lactation: Verapamil crosses the placental barrier and can be detected in umbilical vein blood at delivery. Verapamil hydrochloride/metabolites are excreted in human milk. Limited human data from oral administration has shown that the infant relative dose of verapamil is low (0.1-1% of the mother's oral dose). A risk to the newborns/infants cannot be excluded. Due to the potential for serious adverse reactions in nursing infants, verapamil should only be used during lactation if it is essential for the welfare of the mother.
The following adverse events reactions have been reported with verapamil from clinical studies, postmarketing surveillance or Phase IV clinical trials and are listed as follows by system organ class. Frequencies are defined as: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000); not known (cannot be estimated from the available data).
The most commonly reported adverse drug reactions were headache, dizziness, gastrointestinal disorders: nausea, constipation and abdominal pain, as well as bradycardia, tachycardia, palpitations, hypotension, flushing, edema peripheral and fatigue. (See Table 1.)
 Click on icon to see table/diagram/image
Reporting of suspected adverse reactions:
Click on icon to see table/diagram/image
Reporting of suspected adverse reactions: Reporting of suspected adverse reactions is an important way to gather more information to continuously monitor the benefit/risk balance of the medicinal product.
In vitro metabolic studies indicate that verapamil hydrochloride is metabolized by cytochrome P450 CYP3A4, CYP1A2, CYP2C8, CYP2C9 and CYP2C18. Verapamil has been shown to be an inhibitor of CYP3A4 enzymes and P-glycoprotein (P-gp). Clinically significant interactions have been reported with inhibitors of CYP3A4 causing elevation of plasma levels of verapamil hydrochloride while inducers of CYP3A4 have caused a lowering of plasma levels of verapamil hydrochloride, therefore, patients should be monitored for drug interactions. Co-administration of verapamil and a drug primarily metabolized by CYP3A4 or being a P-gp substrate may be associated with elevations in drug concentrations that could increase or prolong both therapeutic and adverse effects of the concomitant drug.
The following table provides a list of potential drug interactions due to pharmacokinetic reasons: (See Table 2.)
Click on icon to see table/diagram/image
Other Drug Interactions and Additional Drug Interaction Information: HIV antiviral agents: Due to the metabolic inhibitory potential of some of the HIV antiviral agents, such as ritonavir, plasma concentrations of verapamil may increase. Caution should be used or dose of verapamil may be decreased.
Lithium: Increased sensitivity to the effects of lithium (neurotoxicity) has been reported during concomitant verapamil hydrochloride-lithium therapy with either no change or an increase in serum lithium levels. The addition of verapamil hydrochloride, however, has also resulted in the lowering of the serum lithium levels in patients receiving chronic stable oral lithium. Patients receiving both drugs should be monitored carefully.
Neuromuscular blockers: Clinical data and animal studies suggest that verapamil hydrochloride may potentiate the activity of neuromuscular blocking agents (curare-like and depolarizing). It may be necessary to decrease the dose of verapamil hydrochloride and/or the dose of the neuromuscular blocking agent when the drugs are used concomitantly.
Acetylsalicylic acid: Increased tendency to bleed.
Ethanol (alcohol): Elevation of ethanol plasma levels.
HMG Co-A Reductase Inhibitors ("Statins"): Treatment with HMG CoA reductase inhibitors (eg. simvastatin, atorvastatin or lovastatin) in a patient taking verapamil should be started at the lowest possible dose and titrated upwards. If verapamil treatment is to be added to patients already taking an HMG CoA reductase inhibitor (e.g. simvastatin, atorvastatin or lovastatin), consider a reduction in the statin dose and retitrate against serum cholesterol concentrations. Fluvastatin, pravastatin and rosuvastatin are not metabolized by CYP3A4 and are less likely to interact with verapamil.
Antihypertensives, diuretics, vasodilators: Potentiation of the hypotensive effect.
Shelf Life: 3 years.
Store the drug carefully at or below 25°C.
C08DA01 - verapamil ; Belongs to the class of phenylalkylamine derivative selective calcium-channel blockers with direct cardiac effects. Used in the treatment of cardiovascular diseases.
Isoptin SR tab 240 mg
30's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image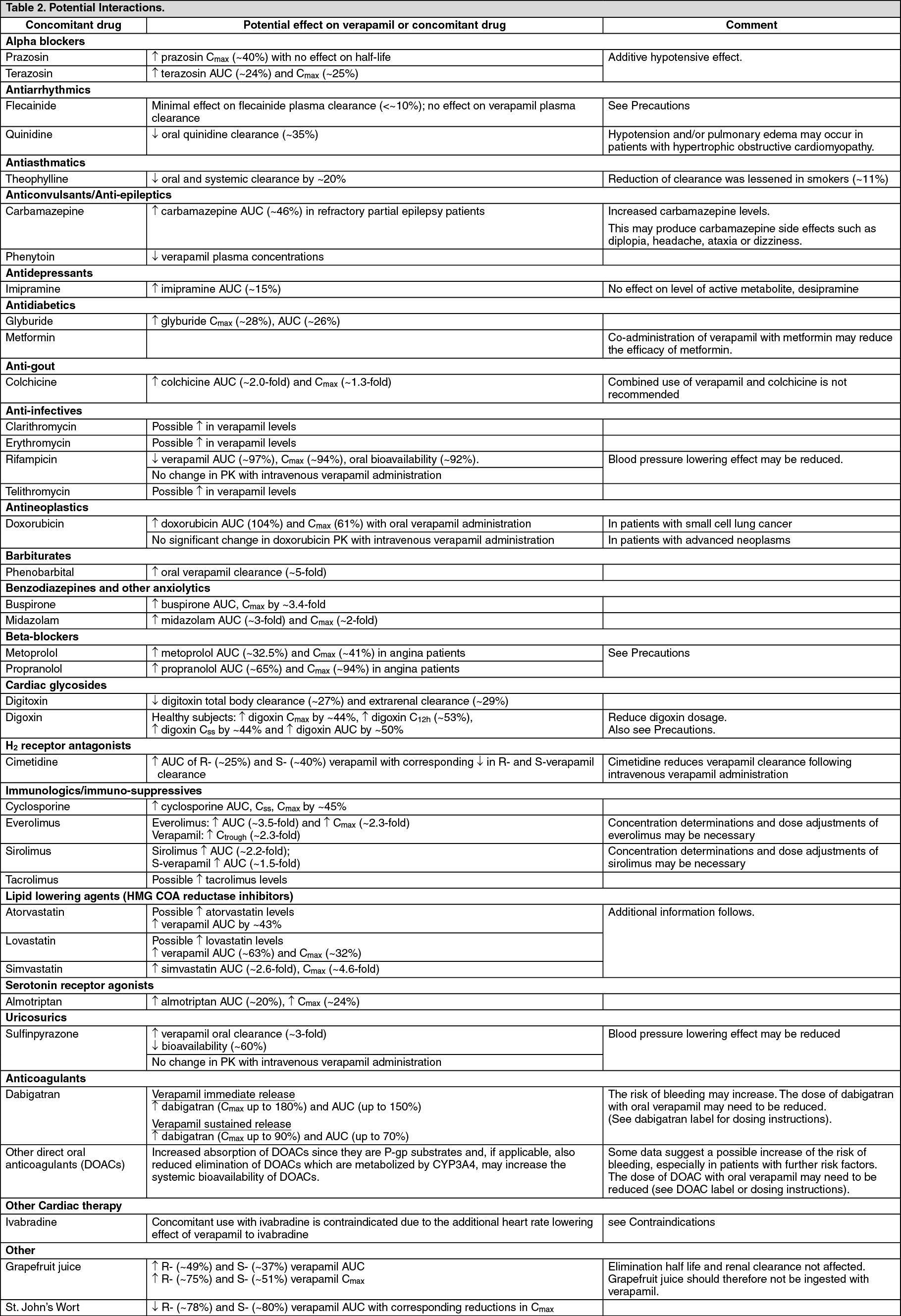 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
